

This guide explains the science behind Colourstart® as a universal screening test for allergy to oxidative (permanent) hair colourants, with a focus on p‑phenylenediamine (PPD) and related dye ingredients.
It is written for hairdressers, salon owners, colour educators, manufacturers, insurers and other stakeholders who want a deeper, evidence‑based understanding of the product function as a universal hair colour allergy test.
It brings together independent dermatology literature, real‑world Colourstart data, and public positions from regulators (including the Medicines and Healthcare products Regulatory Agency - MHRA) and industry bodies to show why a PPD‑based patch test can act as a practical universal screen for oxidative hair colour allergy.

Oxidative hair colourants are a recognised cause of allergic contact dermatitis (ACD). The main culprit is PPD, but closely related aromatic amines such as p‑toluenediamine (PTD), 2‑methoxymethyl‑PPD (ME‑PPD or ME+), p‑aminophenol (PAP) and m‑aminophenol (MAP) are also implicated.
Epidemiological data show that hair dye allergy is not rare. In the EDEN study1, which included over 10,000 healthy adults (2,739 patch‑tested), the approximate prevalence of PPD contact allergy was 0.8%. Use of black henna tattoos, which often contain illegally high concentrations of PPD, was strongly associated with later reactions to oxidative hair dye.
For hairdressers and their stakeholders, the key point is that while most clients will never experience a skin reaction, allergy to oxidative hair dye is common enough, and serious enough for legislation to require products containing these ingredients to be labelled with special warnings. It is sensible to give hairdressers and their clients access to a product to help manage these risks proportionately.
Within the professional hairdressing supply chain, there is a persistent misconception that some oxidative hair colours are effectively “PPD‑free2” in a way that removes allergy risk. In reality, most permanent oxidative dyes rely on a family of closely related para‑amines, of which PPD is the best‑known example, such as PTD or ME+.
Dermatologists worldwide include PPD (typically 1% in petrolatum) in the baseline patch test series as an index allergen for oxidative hair‑dye allergy diagnosis. In other words, PPD is widely used clinically as a marker allergen: if a patient reacts to PPD, this is taken as a strong indication of allergy to the broader group of para‑amine hair dyes. This is why PPD is so important3 in both clinical diagnosis and (salon) screening, even when a given hair colour product does not list “PPD” on the label but instead contains closely related substances.

In 2019, Colourstart became the first and only MHRA‑licensed cutaneous patch test4 for screening allergy to PPD in consumers aged 16 years and over.
To obtain this licence, Colourstart had to demonstrate:
Recognised by all major UK hair and beauty trade organisations and designed specifically for professional use, Colourstart gives hairdressers a consistent, regulated standard for managing colour allergy risk — not diagnosing it. No screening test is a perfect predictor of allergic contact dermatitis. Colourstart identifies those most at risk from the principal sensitising allergen family in oxidative hair colour while minimising the risk of active sensitisation, a risk that increases with every repeated allergen exposure.
See section 10.
Since licensing, Colourstart has been used extensively by salons and consumers, and real‑world data have been presented twice at Congresses of the European Society of Contact Dermatitis (ESCD).
Two key datasets have been published.
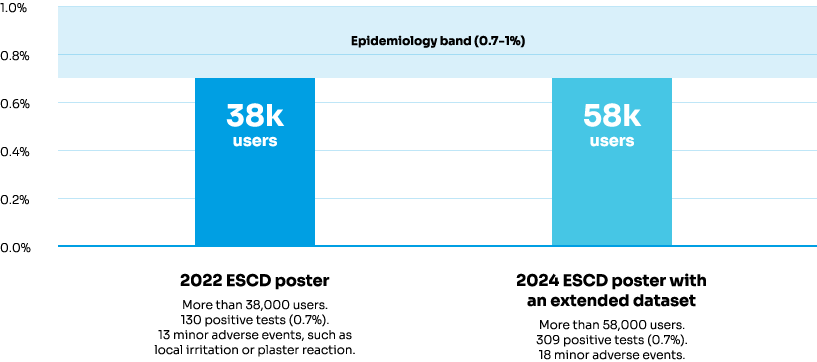
The positive rate of 0.7% is remarkably consistent across datasets and aligns well with European epidemiological estimates of PPD allergy prevalence (around 0.7–1%). Adverse events were rare, mild and non‑serious, and in the 20225 and 2024 datasets6, a pre‑screening questionnaire was used to identify individuals already highly likely to be allergic to hair dye; these consumers were advised not to apply the patch.
In practice, this suggests that Colourstart is detecting approximately the proportion of clients one would expect to be allergic to PPD based on independent studies, while the safety profile in large‑scale use has been very favourable.
Allergic contact dermatitis to hair dyes does not exist in isolation for each separate ingredient. Many of the oxidative dye intermediates are structurally similar para‑amines, and the immune system can cross‑react between them.
Multiple studies have shown strong cross‑reactivity between PPD and other oxidative dye ingredients3. A PPD test identified 80.7–86.8% of people already known to be allergic to PTD, m-aminophenol, or p-aminophenol.
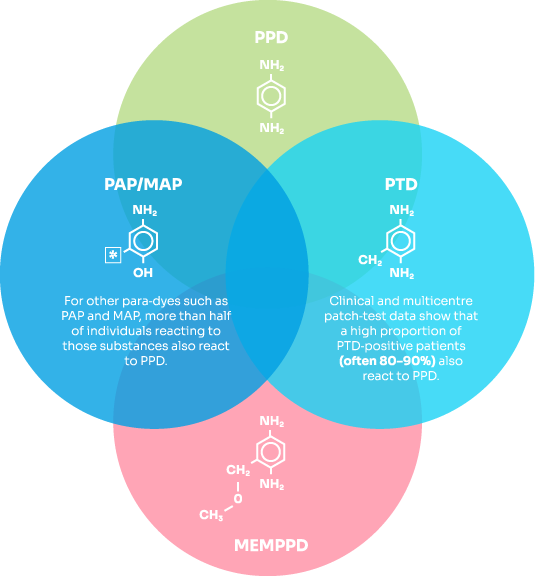
Taken together, these findings support the view that PPD allergy serves as a reliable marker7 for allergy to the broader family of oxidative hair‑dye intermediates.
For hairdressers, this means that replacing PPD with another para‑amine such as PTD or PAP does not remove the underlying allergy risk for PPD‑allergic clients; it simply exposes the client to a slightly different allergen within the same reactive family. It is worth remembering that the clinical advice is clear: “Advice for patients with hair dye allergy remains stop using permanent hair dyes8”.
ME‑PPD (also known as ME+) has been introduced as a lower‑potency allergen alternative to PPD in some oxidative hair colour formulations.*
Human studies in PPD‑allergic individuals show that:
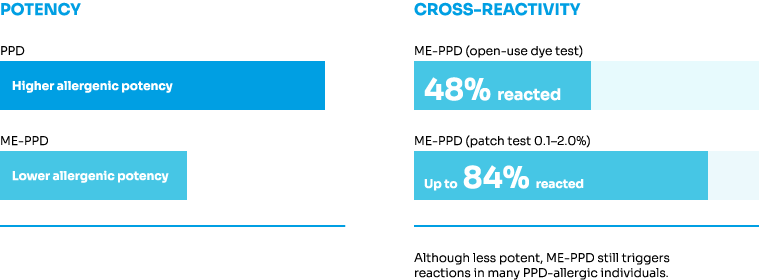
* Potency reduction is only demonstrated in a mouse model.
These results indicate that although ME‑PPD is less potent than PPD, it is clearly cross‑reactive and should not be assumed to be safe for PPD‑allergic individuals. From a screening perspective, this supports the continued use of PPD as a relevant marker allergen, even for products formulated with ME‑PPD instead of PPD.
In recent years, “PPD‑free” claims have been used in marketing some oxidative hair colours. However, these products may still contain PPD‑related para‑amines, and regulators have taken a clear stance on this.
In 2025, the UK Advertising Standards Authority (ASA) ruled on advertising10 for a hair‑colour range described as “PPD‑free” while containing PTD.
The ASA concluded that:
The Cosmetic, Toiletry and Perfumery Association (CTPA), the UK trade association for cosmetics and personal‑care companies, has issued guidance11 on “PPD‑free” claims which states that:
| PROPERTY | PPD | PTD | PAP/MAP | ME-PPD |
|---|---|---|---|---|
| CAS number | 106-50-3 | 95-70-5 | 123-30-8 | 337906-36-2 (base); 337906-37-3 (sulfate) |
| Chemical formula | C6H8N2 | C7H10N2 | C6H7N0 | C8H12N2O |
| Required pictograms | ||||
| Signal word | Danger | Danger | Warning | Danger |
These public statements are consistent with the dermatology literature on cross‑reactivity and reinforce the need for honest, precise communication about allergenic para‑amines in hair colour products.
Most oxidative hair colour manufacturers recommend a 48‑hour Allergy Alert Test (AAT) before use. Dermatology literature has discussed these tests critically12, raising several concerns:
These limitations mean that AATs are not equivalent to a standardised, regulated screening tool, and they may themselves carry sensitisation risk13 when used repeatedly with high‑dose dye mixtures.
While UK salons adopted Colourstart primarily for practical reasons, industry stakeholders should also understand the scientific concerns surrounding manufacturer Allergy Alert Tests:
From a professional liability perspective, there is also a practical issue around who performs allergy tests. With Colourstart, the client applies the test themselves and, by completing the associated questions, self‑certifies their suitability for colour. This keeps the allergy decision with the client and the licensed medicine, rather than relying on hairdressers to interpret skin reactions, and avoids the additional complexity of the Allergy Alert Test, where irritant reactions to components of the colour formulation can be difficult to distinguish from true allergy.

Taken together, the evidence leads to several clear conclusions:

For hairdressers and their stakeholders, this provides the context for using Colourstart as a PPD‑based universal screening test for individuals considering oxidative hair colouring. It offers a regulated, standardised way to screen for relevant allergy across the para‑amine dye family, supports professional duty of care, and can be integrated into salon protocols in place of, or alongside, traditional AATs.